
|
|
Assalamualaikum dan Salam Sejahtera
Di antara subjek yang tidak diberi penekanan yang mencukupi di dalam kurikulum perubatan ialah nutrisi dan sains/perubatan sukan. Ada yang berpendapat subjek-subjek tersebut lebih sesuai ditangani pada tahap pasca ijazah. Apapun, hakikatnya ialah sebagai pengamal-pengamal perubatan kita sering didampingi untuk mendapatkan nasihat darihal perkara-perkara tersebut.
Sempena dengan Kuala Lumpur
1998, Sukan Komanwel ke 16 bulan ini, Buletin CME memberi tumpuan khas
kepada isu-isu yang berkait rapat dengan kesukanan dan nutrisi sukan.
Universiti Sains Malaysia, sejak penubuhan Pusat Pengajian Sains Perubatan
telah banyak memainkan peranan ke arah menyumbang kepada pengetahuan dalam
bidang sains sukan. Pada tahun ini, USM mencatatkan sejarah
sebagai universiti pertama di Malaysia menganjurkan Kursus Sains Sukan
dan Perubatan Sukan pada tahap pasca ijazah. USM juga mendapat pengiktirafan
dengan penubuhan Pusat Kawalan Doping di kampus induk. Diharapkan dengan
usaha USM ini akan lahirlah ramai tenaga berketerampilan yang sekaligus
akan menyumbang kepada kecemerlangan yang berterusan dalam dunia sains,
perubatan dan kesukanan
Sekian, terima kasih.
Prof.
Madya Dr. Abdul Rashid Abdul Rahman
Editor
![]()
|
|
|
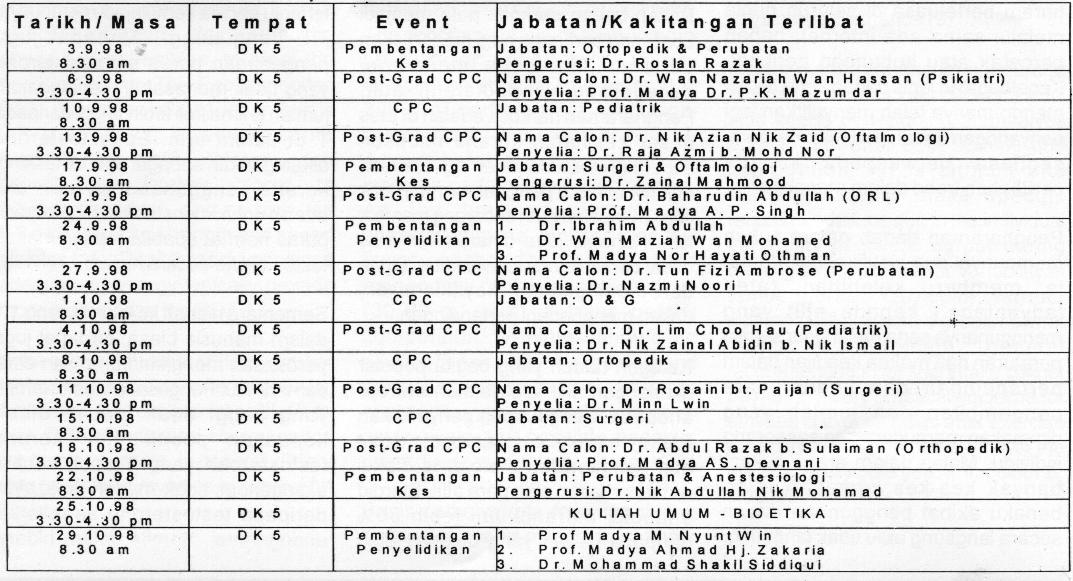
3 - 15 October 1998 |
|
Biostatistic and Research Methodology;
17 - 29 October 1998 |
![]()
| . |
THE
INTEGRATED MASTER OF SCIENCE PROGRAMME FOR SPORTS SCIENCE AND SPORTS MEDICINE
AT UNIVERSITI SAINS MALAYSIA
 |
Assoc. Prof.
Mafauzy Mohamed
BSK, MBBS (Adel), MRCP (UK) M.Med. Sc. (Sheffield) FRCP (Edin) Dean School of Medical Sciences |
 |
Assoc. Prof.
Rabindarjeet Singh
BSc (Hons) (Essex), PhD (London) Sports Science Course Coordinator |
 |
Dr. Nordin Simbak,
MD (UKM), M.S. (Ortho, UKM) Sports Medicine Course Coordinator |
The reform in medical education curricula over the past few decades have been initiated partly as a response to the changing needs of society and partly because of the participation of medical educators in expanded opportunities for educational development. In this aspect, the School of Medical Sciences at Universiti Sains Malaysia, took a major step and introduced an integrated medical curriculum in 1980 which had both horizontal and vertical integration with appropriate assessment tools.
As the educational curricula experienced great changes over the past few decades, the same is seen in the sports scene in Malaysia which has witnessed a rapid expansion over the last few years. This rapid expansion is in part due to the introduction of professionalism in sports and the increased awareness of the importance of physical exercise in health.
The one aspect that could significantly contribute to the development of sports in this country is the role of sports sciences in both educational and applied aspects of sports. With this recognised need of the educational aspect of sports science, the School of Medical Sciences at Universiti Sains Malaysia has taken the initiative of establishing an innovative integrated Masters of Science programme for Sports Science and Sports Medicine which envisages the graduates to acquire the expertise needed to contribute to the expanding field of sports, health and recreation. The aim of the course is to enable physical educators, instructors, coaches, health-care professionals (nutritionists, physiotherapists, fitness leaders and community health providers) and medical doctors to gain knowledge and develop skills in the field of sports science, exercise physiology and sports medicine.
Course Structure
The curriculum is designed to enable graduates
of the Sports Science course to demonstrate a knowledge of:-
1) the basic sciences which are relevant
for understanding the relationship between health and exercise
2) the health benefits of exercise
3) exercise training, nutrition evaluation
and conducting a fitness assessment
4) the psychological aspects of competitive
sports
In addition to the above three objectives, the Sports Medicine graduates will also acquire:-
5) an ability to assess and understand
the principles of:
a) prevention
and rehabilitation of sports injuries
b) rehabilitation
of persons suffering from life-style diseases.
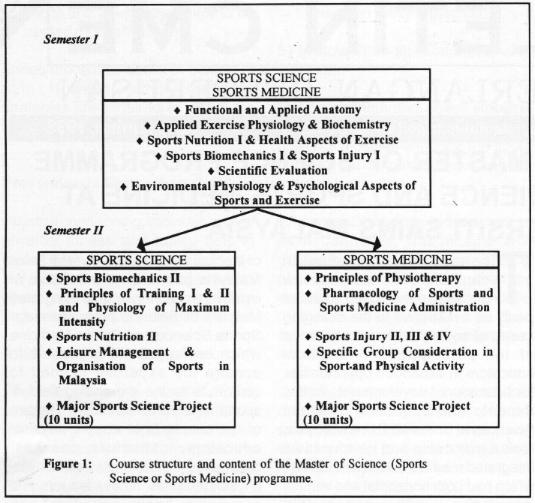
The integrated curriculum, which runs over one academic year, will be taught over two semesters (see Figure 1). The first semester will have core modules which will be taken by both the Sports Science and Sports Medicine students, with the students separating into the Sports Science and Sports Medicine modules in the second semester.
Wherever possible, an attempt has been made to link certain core modules as shown in Figure 1. One such example is linking Sports Biomechanics to Sports Injuries and prevention of injuries. This approach to biomechanics is important as it may be termed as kinesiology in contrast to the mathematical description of human movement, or in other words, it may also be described as functional anatomy.
Apart from the coursework, students in both majors (Sports Science and Sports Medicine) will be required to submit a dissertation of about 15,000 words, which would form 25% of the course time. The work must address a clearly-identified problem that would be chosen and students would be required to show evidence of familiarity with relevant literature, appropriate experimental design and methodology and satisfactory interpretation of the results. In this aspect, the Sports Medicine students will team up with Sports Science students to overcome the library-based/record-based projects by students of Sports Medicine as experienced in some courses in other countries.
Conclusion
With this innovative and integrated Masters
of Sports Science and Masters of Sports Medicine programme, it is intended
that the graduates from these courses will acquire the expertise needed
to contribute to the expanding field of sports, health-care, and recreation.
This will help fulfill the nations needs in this era of professionalism
and improve the healthy living standards of Malaysians. By offering
this course, Universiti Sains Malaysia will be the centre of excellence
for providing knowledge on health-care, fitness and sports science.
|
|
PENYALAHGUNAAN
DADAH DALAM SUKAN
 |
Prof. Madya Dr.
Aishah A. Latiff
Pengarah Pusat Kawalan Doping Universiti Sains Malaysia |
Perkataan doping daIam sukan merujuk kepada penggunaan dadah/ubat yang diharamkan oleh International Olympic Council (IOC), bagi tujuan mendapatkan kelebihan daIam prestasi atlit. Doping dalam abad-abad kebelakangan ini telah menjadi sebutan dan amalan atlit profesional mahupun amatur dan ini telah menambahkan lagi cabaran bagi pihak makmal dalam pengesanan dan penganalisaan dadah-dadah ini. OIeh kerana atlit sentiasa mencari kelebihan untuk mengejar kemenangan, edaran dadah secara haram berIeIuasa di seluruh dunia melalui sama ada internet, bahan bercetak atau hubungan peribadi. KepeIbagaian jenis dadah serta teknik menggunanya telah menyulitkan lagi penyaringan dadah dan makmal perlu sentiasa berwaspada kepada perubahan trend dalam masalah ini.
Pengharaman
dadah dalam sukan mempunyai dua justifikasi; pertama, ia memberi kelebihan
(atau advantage) kepada atlit yang menggunanya serta melanggar segala
peraturan dan makna keadilan dalam pertandingan dan kedua, cara pengambilan
dan jumlah yang digunakan memudaratkan seseorang individu. Malah dalam
arena sukan, banyak kes-kes kematian teIah berlaku akibat penggunaan dadah
secara langsung atau tidak langsung.
Dadah
yang diharamkan oleh IOC
Diantara dadah-dadah lama yang telah digunakan sejak awaI 1970an adalah perangsang (stimulant) dan narkotik. Tujuan penggunaan stimulant begitu nyata kerana bahan seperti amfetamin memberi tenaga serta ketahanan yang amat baik terutama dalam pertandingan seperti lumba basikal, Iarian jarak jauh, acara renang, semuanya yang memerIukan daya tahan. Kini senarai dadah yang digunakan bagi tujuan di atas telah berlipat ganda dan kini makmal perlu mengesan sejumlah 70 jenis dadah perangsang. Tambahan pula, bahan seperti kafein, ephedrine, pseudoephedrin menyulitkan lagi kawalan kerana bahan ini terdapat dalam pelbagal minuman dan makanan dan juga ubat-ubatan over-the counter untuk pelbagai rawatan. Oleh yang demikian bahan-bahan ini perlu dinilai jumlahnya di dalam urin; jumlah kafein melebihi 12 mg/mI di dalam urin misalnya akan dirumuskan sebagal positif. Paras ini diketahui dapat dihasilkan oleh pengambilan kafein sahaja dan tidak akan tercapai meskipun atlit telah minum beberapa cawan kopi pekat.
Bahan-bahan narkotik pula menjadi ubat yang berkesan bagi meneruskan pertandingan tanpa menghirau kecederaan yang diaIami atlit. Pengharaman narkotik adalah di atas dasar kesihatan kerana tindakan seperti ini memudaratkan lagi keadaan atlit. Selain itu, penggunaan narkotik tidak mendatangkan sebarang manfaat lain. Kanabis juga diharamkan atas dasar bahan ini membawa ketenangan dan meningkatkan keyakinan diri dalam menghadapi pertandingan.
Kategori dadah yang begitu popular dikaIangan atlit ialah bahan steroid anabolik. Sungguhpun penyeIidikan tidak menunjukkan sebarang manafaat dari pengambilan steroid, ia diakui amat berkesan oleh para atlit. Steroid anabolik merangkumi Iebih 50% daripada dadah yang dikesan oleh makmal-makmal doping seIuruh dunia. Perkara ini telah membuka peIbagai peluang penyeIidikan kerana penganalisaan dadah sintetik semakin rumit dan segi spesifisiti dan sensitiviti manakala pengesanan hormon steroid seperti testosterone, DHT (dihydrotestosterone) dan DHEA (Dehydroepiandrosterone) memerlukan interpretasi yang begitu cermat kerana mereka juga merupakan hormon yang terdapat semuIajadi dalam badan manusia. OIeh yang demikian pelbagai kriteria teIah dibangunkan bagi memutuskan urin yang positif. Suatu parameter yang dinilai adalah nisbah testosterone (T) kepada epitestosterone (E), suatu hormon berkaitan tetapi tidak menghasilkan sebarang kesan. Penggunaan testosterone akan mengubah paras T dan tidak menjejas paras E. Perkara ini mengujudkan T:E yang tinggi; malah urin yang menunjukkan T:E melebihi 6 akan disiasat dengan lebih mendalam. Penganalisaan semula akan dilakukan ke atas urin yang dikumpul semula dan atlit yang sama apabila angka ini jatuh diantara 6 dan 10. Tindakan ini adalah bagi mempastikan atlit benar-benar menggunakan testosterone kerana terdapat juga individu-individu tertentu secara semulajadi mempunyai T:E yang tinggi. Terdapat juga pengesanan paras epitestosterone yang tidak munasabah sehinggakan jumlah E lima kali Iebih tinggi daripada T di dalam urin. Epitestosterone dikategorikan sebagai agen masking kerana penggunaannya oleh atlit adalah untuk menstabilkan T:E kepada paras normal apabila menggunakan testostorone secara haram.
Sementara nisbah ini lebih kurang 1:1 dalam manusia biasa, terdapat juga perbezaan mengikut kumpulan etnik dan individu. Pengesanan testosterone yang tinggi tidak mudah diberi kepastian positif oleh kerana testosterone yang diambil secara eksogenous tidak mudah dibezakan daripada testosterone semulajadi endogenous. Saintis dalam bidang analisis doping sedang menyelesaikan isu ini melalui penentuan isotop stabil karbon, 12C dan 13C dalam testosterone. Ini adalah berdasarkan nisbah 12C : 13C dalam testosterone eksogenous jauh berbeza daripada testosterone semulajadi. Nisbah ini pula bergantung kepada diet masing-masing. Penentuan ini hanya dapat dilaksanakan melalul suatu teknik yang menggunakan alat Gas Chromatograph Isotope Ratio Mass Spectrometer, suatu alat yang memberi fingerprint kepada bahan kimia melalui kandungan isotopnya.
Selain parameter yang dikesan melalui penganalisaan, perubahan fisikal begitu ketara pada pengguna steroid anabolik. Bagi lelaki, perubahan otot yang bertambah, kehiIangan rambut, pertumbuhan buah dada dan masalah akne begitu ketara manakala bagi wanita, terdapat tumbuhan rambut di beberapa bahagian badan termasuk muka serta perubahan suara yang semakin kasar.
Steroid anabolik adalah bahan yang digunakan di luar masa pertandingan oleh kerana manafaatnya serta perubahan yang diingini pengguna didapati semasa latihan. Oleh yang demikian pengesanan positif sering didapati apabila program kawalan di luar pertandingan dijalankan; beberapa bulan sebelum pertandingan penggunaannya dihentikan bagi mengelak pengesanan. Oleh kerana eIiminasi steroid begitu berpanjangan dalam badan manusia, kehadirannya masih kadangkala dapat dikesan dalam paras ppb (parts per billion) beberapa bulan selepas tamat penggunaan. Keupayaan mengesan paras sekecil ini dituntut oleh pihak lOC dan makmal kini perlu ada kemampuan mengesan beberapa jenis steroid sehingga ke tahap sekecil 1-2 ng/mI. Ini bermakna teknik seperti tandem mass spectrometry (MS/MS) atau high resolution mass spectrometry (HRMS) terpaksa digunakan. Teknik-teknik ini akan memberi lebih sensitiviti tanpa berkompromikan spesifisiti. Sukan OIimpik di Atlanta merupakan kali yang pertama pengesanan menggunakan HRMS dilakukan supaya threshhold pengesanan yang begitu rendah dapat dilaksanakan. Buat masa ini teknik tersebut telah dibangunkan bagi sejumlah kecil steroid tetapi malangnya, alat yang digunakan terlalu mahal.
Suatu kelas dadah yang diharamkan oleh lOC adalah agen diuretik yang menjadi pilihan atlit dalam usaha menghapuskan kesan-kesan dadah steroid menjelang pertandingan sukan. Melalui cara ini paras steroid dapat dikurangkan di bawah paras threshold pengesanan. Ini semakin penting bagi atlit oleh kerana makmal doping seluruh dunia kini lengkap dengan alat yang dapat mengesan dalam tahap ppb (parts per billion). Selain itu mengurangkan air di dalam badan memberi manafaat kepada bidang sukan yang menggunakan berat badan sebagal kriteria. Dalam acara angkat berat misalnya, seorang peserta mungkin dapat dimasukkan ke dalam kategori yang lebih rendah.
Ubat darah tinggi yang dikenali sebagal penghalang-beta juga disalahgunakan oleh atlit dalam acara-acara sukan seperti memanah, menembak, dan bidang sukan yang memerlukan penumpuan seseorang. Objektif pengunaan adalah untuk mengurangkan tremor dan kegugupan yang mungkin berlaku. Senarai ini termasuk jenis yang sering digunakan oleh pesakit seperti metoprolol hingga yang jarang digunakan seperti pindolol dan bisoprolol.
Cabaran terbaru bagi pihak penguasa adalah untuk mengesan hormon peptida. Ini termasuk hCG (human chorionic gonadotropin), eritropoietin (EPO) dan hormon pertumbuhan (hGH). Sungguhpun yang pertama diantara tiga bahan ini dapat dikesan di dalam urin, dua lagi hanya dapat dlkesan di dalam serum darah. OIeh kerana peraturan kawalan doping hanya membenarkan pengambilan sampel urin, EPO dan hGH belum dapat dinilai. Tambahan pula kaedah pengesanan masih terhad kepada teknik ElA (enzyme immunoassay) dan RIA (radioimmunoassay) yang boleh diterima sebagai kaedah penyaringan tetapi belum lagi ujud kaedah ujian evidentiaI yang tidak boleh dipertikaikan dalam mahkamah. Kaedah EIA dan RIA mungkin selektif atau spesifik tetapi satu kaedah sahaja tidak memberi tahap diskriminasi yang dituntut seperti dengan menggunakan mass spektrometri. Sementara penggunaan EPO dan hGH nyata mempunyai sebab-sebab tertentu, hCG biasanya mula diambil setelah tamat regimen steroid untuk merangsang semula hasilan testosterone endogenous. Beberapa jenis EPO sintetik didapati di pasaran dengan hasilan kesannya sama seperti peningkatan hasilan sel darah merah ke tahap 5-10 kali ganda kadar normal. Malangnya, dengan jumlah sel merah yang melambung tinggi, darah menjadi likat sehingga jantung seseorang boleh terhenti dalam kepenatan bertanding. Penyelidik percaya EPO telah menyebabkan 18 kematian di kalangan peIumba basikal Belanda dan Belgium sejak tahun 1987.
Kaedah doping
Selain daripada senarai dadah-dadah yang diharamkan oleb pihak IOC, terdapat juga kaedah doping yang dilarang. Ini tidak melibatkan bahan asing tetapi merupakan manipulasi untuk meningkatkan prestasi melalui doping darah atau penipuan untuk mengelakkan daripada dikesan di dalam urin.
Objektif melakukan doping darah adalah serupa dengan hasil penggunaan EPO. Melalui kaedah ini seorang atlit akan mengeluarkan Iebih kurang 200-250 ml darah dan dikembaIikan semula sel darah merah ke dalam sistem badannya 4-6 minggu kemudian sebelum bermulanya pertandingan. Cara mi meningkatkan hematokrit dan tidak secara langsung bekalan oksigen juga ditingkatkan untuk tujuan mendapatkan tenaga maksimum dan memperlanjutkan ketahanan. Nyata bahawa proses seperti ini akan melibatkan beberapa orang selain atlit kerana darah perlu diproses secara profesional.
![]()
|
|
EXERCISE
FOR HEALTH
 |
Assoc. Prof. Roland
Sirisinghe,
MBBS (Colombo), MRCP (UK) Department of Physiology |
Physical Activity and Health
The link between physical activity and health had been proposed over two thousand years ago, but only relatively recently have studies demonstrated unequivocally the health benefits of physical activity. Physical activity is now known to prevent and/or retard the progression of several diseases; among them are hypertension, ischaemic heart disease, stroke, diabetes mellitus, osteoporosis, some arthritides, obesity, hyperlipidaemia, several malignancies, major depression and anxiety states. An equally important but often forgotten benefit is the slowing of the ageing process. Unfortunately, however, less than 50% of individuals seem to take part in sufficient physical activity to have a positive influence on their health. Health authorities world wide now recommend that all adults take part in sufficient physical activity to derive the health benefits
Goals of Activity Recommendations
The initial recommendations for exercise were directed towards improving cardiovascular fitness. Subsequently, however, it was realised that health benefit derived is not entirely through better cardiorespiratory function. For example improved muscle strength and flexibility, increased insulin sensitivity and mental effects of exercise all contribute towards health, but these effects do not necessarily occur in parallel with improvement in cardiorespiratory function. Thus current recommendations seek to improve more than just cardiorespiratory fitness: but aim to reduce mortality from various causes and also to enhance ones ability to undertake daily living activities.
Activity Recommendations
The most recent and widely
cited recommendations are those jointly issued by the Centers for Disease
Control and Prevention and the American College of Sports Medicine. They
recommend, for adults, that the minimum activity level should constitute
· moderate intensity
physical activity.
· a total duration
of 30 minutes daily (which can be in one continuous session or in two or
three discontinuous sessions)
· daily activity
or at least 6 days a week
Intensity - Moderate
activity is defined as such activities that expends 3-6 METs (MET - metabolic
equivalent; the energy spent by an individual per unit time during sitting
at rest; approximately 1.5 Kcal/min. in an adult). Such activities include
· brisk walking (6.4
Km/hr)
· recreational cycling
· child care e.g.
walk, run and play with child
· swimming with moderate
effort
· mowing lawn
There is considerable evidence to show that moderate activity confers almost the same overall health benefits as vigorous activity although the cardiorespiratory function improves more with the latter.
How does one determine if the activity is of sufficient intensity? The Talk Test is a user-friendly assessment tool. The intensity is sufficient if during exercise, one is able to carry on a conversation with some laboured breathing, but exertion should never be so intense that one cannot talk. On the other hand if one can carry on unlimited, unlaboured discussions while exercising, the intensity needs to be increased.
Duration - The concept of similar health benefits from continuous exercise and discontinuous exercise of the same total duration is a recent one and is based on both epidemiological and intervention studies. This means that individuals who engage in short spurts of activity during work or leisure stand to benefit from them. This may also make it more convenient for the individual to fit in a period of such activity at work or interspersed among other duties.
Frequency - Some benefits of exercise are short-lived. Increased insulin sensitivity and post prandial lipaemic control are two examples. The effect of exercise on the former seems to last 36-48 hours while that of the latter lasts only about 24 hours. Thus to derive maximum benefit exercise must ideally be repeated at least every 24 hours.
It must be emphasised that the above are minimum recommendations. Those whose physical activities exceed the guidelines above should maintain them. Indeed even these individuals, other than those at the highest level of activity, should attempt to increase the intensity and/or frequency of activity if possible, but not at the expense of suffering injuries or other ill effects. In the event that further increase is not possible, the aim would also be to maintain the activity in the long term
Exercise at Individual Level
While the general aims and recommendations hold true for all individuals, the existence of differences among individuals means that advice for any one person needs to be individualised.
The activity recommended should obviously be effective but should also be safe for the individual and he or she should have the necessary facilities and should be able to be compliant and adhere to the programme in the long term. The intensity that is only moderate and short sessions expand the spectrum of possible choices.
It has been shown that the
success of an exercise programme increases when
· it is more individualised
than regimental
· it is based on
a persons existing daily activities and schedule rather than a completely
new item
· it could be carried
out within ones existing environment than at a special facility
The exercise pyramid has been proposed for those who have previously been sedentary. At level one of the exercise pyramid a higher level of activity is achieved through routine daily work. This could be in the form of additions to daily tasks e.g. taking the stairs to the office instead of the lift, parking the car further away from the supermarket, or increasing the intensity of existing activities e.g. cleaning the house at a faster pace. One may also increase the pace at which one moves about in the house, garden or the workplace. When daily tasks are considered as components of an activity programme it must be emphasised that it not merely carrying out the task that is important but doing it at the agreed pace.
In the second level, short bouts of extra activities may be incorporated into the daily routine. Ideally these should merge easily with the individuals daily programme. e.g. a 10 minute brisk walk or cycling. These activities are mostly aerobic at a moderate pace. The activities for the first and second levels develop aerobic capacity and are to be daily or at least on 6 days of the week.
At level three are additional recreational sporting activities. The aim is to further improve cardiorespiratory fitness and increase muscle strength and joint flexibility. It often goes unrealised that exercises for health commonly practiced (walking, jogging, cycling) involve mostly the lower body whereas much of ones daily activities involve the upper body and require muscle strength and flexibility rather than aerobic fitness. Incorporation of recreational sports, for example racquet sports, golf or swimming on about 3 days a week aims to redress this incongruity. If facilities are available, systematic weight training or resistance exercises using a suitable apparatus on 2-3 days of the week is recommended. Some household activities like gardening also help to strengthen the upper body.
Levels one to three may be implemented one after the other at suitable time intervals depending on the individual. The activities in levels two and three should ideally be varied to avoid monotony.
The fourth and the final level of the pyramid is minimising the time spent sitting down. Foremost would be the time spent on watching television and perhaps playing computer games. When ones work requires being seated down, the aim would be to get up and move about every half hour or so.
Starting an exercise programme
Precautions are advised in the case of individuals taking up exercise programmes after many years of sedentary life. As a broad generalisation men under the age of 40 years and women under the age of 50 who are apparently healthy, asymptomatic and have no cardiovascular risk factors need to be subjected to only a medical history and physical examination before starting on an exercise programme. Those over the ages mentioned above or those with cardiovascular risk factors or other chronic illness may need further evaluation, particularly of cardiovascular function. The exact nature of evaluation will depend on the circumstances of each individual.
It is best to build up the intensity of exercise gradually over many weeks up to the intended level. Ideally one should begin activity at a leisurely pace which is continued for the intended final duration. The initial frequency could be alternate days. The pace may be increased gradually at fortnightly intervals at first and weekly intervals later until the intended intensity is achieved.
The importance of stretching and warming up before exercise needs to be emphasised to anyone starting an activity programme. Preferably all muscle groups should be stretched, each stretch being held for about 15 seconds. 5-10 minutes of warming up is well worth spending and bring rich returns in terms of reduced injuries.
It must not be forgotten that there are also situations where exercise may be harmful. Some conditions are contraindications for any type of exertion. Severe uncontrolled hypertension, uncontrolled diabetes mellitus and unstable angina are some such conditions. Other medical conditions necessitate selective prohibition or discouragement of exercise. Swimming in poorly controlled epilepsy, high impact sports in pregnancy and osteoporosis and weightbearing exercises in arthritis (of knee, hips) are examples. Not all symptomatic patients, however, need to be barred from exercise; indeed many would benefit from appropriate exercise.
Comprehensive guidelines on medical evaluation prior to beginning exercise programmes and contraindications to exercise are available(see further reading) and may be referred to when dealing with individual patients.
Conclusion
With the present evidence available, it is mandatory that health personnel encourage and promote physical activity among the public. This should be not only for those who already suffer from conditions that benefit by exercise but also for healthy individuals. The success of exercise promotion depends to a great extent on the degree to which advice is individualised.
Further Reading
![]()
|
|
NUTRITION
FOR SPORTS
|
Assoc. Prof.
Rabindarjeet Singh
BSc (Hons) (Essex), PhD (London) Department of Physiology |
One of the basic conditions necessary to maintain top physical efficiency and performance is optimal nutrition. This concept has been defined not as the consumption of excessive calories which would result in obesity, but as the nutrient intake necessary to maintain optimum physical condition for athletic performance.
Nutritional needs
It is rather difficult to
assess the effect of a single component on physical performance because
of the interference of such variables as motivation, type of work performed
and the wide range of individual responses. However, the performance
of an athlete is largely dependent upon a ready supply of nutrients needed
by the working tissues. Despite understanding the relationship between
nutrition and sports performance, current evidence shows that many athletes
do not make food selections that are in agreement with recommendations
for the enhancement of performance (1-2). The disparity between scientific
recommendations for dietary composition and actual food selection and consumption
by athletes may be bridged by an appropriate nutritional guidance.
Instruction on energy needs and foods that provide appropriate quantities
of both macronutrients (carbohydrate, protein and fat) and micronutrients
(vitamins and minerals) and water are basic for influencing food choices.
Good nutrition can be used effectively in training to influence sports
performance before and after a competition (1-2).
General principles of
nutrition
The nutritional needs of
all athletes include energy, macronutrients, vitamins, minerals and water.
Both male and female athletes require adequate energy from a wide variety
of foods to maintain an appropriate weight for their age. Children
and young adults require energy for both growth and exercise, while older
adults may need to focus on nutrient-dense foods that provide less energy
(3).
Nutrition for training
In general, by virtue of
an athletes high energy expenditure, the athlete in training will require
sufficient energy to support daily training needs and maintenance of body
weight. A vast majority of adult athletes undergoing heavy training
may require more than 13 MJ day-1 (>3000 kcal day-1), depending on the
athletes build and on the amount and quality of training of a particular
sport.
The energy needs of female athletes, may be somewhat lower due to their smaller body mass and less intensive nature of training. In a study by Short and Short (4), female athletes energy intake rarely exceeded 12 MJ day-1. In many cases, female athletes may be trying to reduce energy intake to achieve a lower body weight.
Macronutrient needs for
training
Carbohydrate is the most
important source of energy in an athletes diet and therefore the primary
need for the diet of the athlete in training is to meet the additional
nutrient requirement imposed by the training load.
The energy requirements of training are largely met by oxidation (burning) of fat and carbohydrates. The higher the intensity of exercise, the greater the reliance on carbohydrates as a fuel (5-6). If carbohydrate stores are limited, the intensity of the exercise must be reduced to a level where the energy requirements can be met by oxidation. The primary need, therefore, is for the carbohydrate intake to be sufficient to enable the training load to be sustained. Although the body can store large amounts of fat, the capacity for carbohydrate storage is extremely limited: carbohydrate storage is limited to the muscle and liver, where it is stored as glycogen (7).
During each strenuous training session, substantial depletion of the glycogen stored in the exercising muscles and the liver takes place. If this carbohydrate reserve is not replenished before the next training session, training intensity or duration must be reduced, leading to corresponding decrements in the training response (8-9).
Any athlete training hard on a daily basis can really observe this; if a low carbohydrate diet, consisting mostly of fat and protein, is consumed after a days training, it will be difficult to repeat the same training load on the following day (8-9).
The training diet, therefore, should be high in carbohydrate. It is known that a high carbohydrate diet (70% of energy intake as carbohydrate) can enable runners training for two hours per day to maintain muscle glycogen levels, whereas a progressive fall in muscle glycogen content is observed if the carbohydrate intake is low (8-9).
A dietary carbohydrate intake of 500-600g may be necessary to ensure adequate glycogen resynthesis (10). Although dietitians generally recommend an increased intake of complex carbohydrates for the sedentary individual, these high levels of intake are difficult to achieve without consuming large amounts of simple sugars. Most athletes find that they can only satisfy the requirement for carbohydrate by eating sweets, snacks and other foods rich in simple carbohydrates.
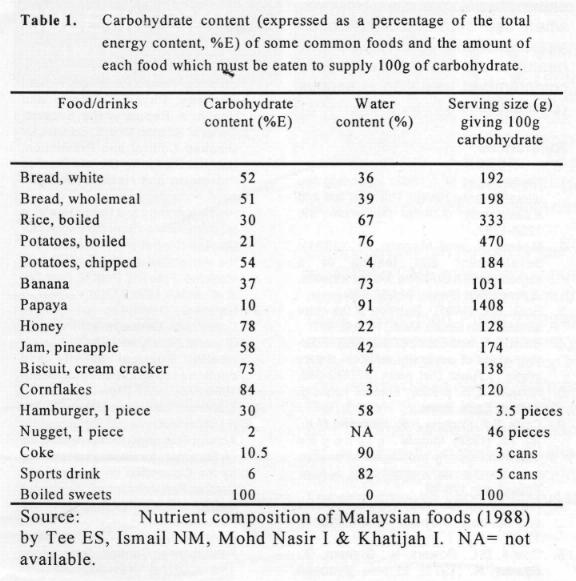
Table 1 shows the carbohydrate content of a variety of foods which might usefully be included in the diet to increase the carbohydrate content.
Along with carbohydrate, adequate protein should be obtained from a selection of meats, dairy products, grains and vegetables, to meet the needs of training. The Recommended Daily Allowance (RDA) for protein is 0.8 g kg-1day-1; however, some researchers feel athletes can benefit from intakes closer to 1.2-1.4 g kg-1day-1 and as high as 1.7 g kg-1day-1 for strength and speed athletes (11). Diets that are varied and adequate in energy typically provide more protein than the RDA.
In the case of fat, most athletes appear to consume adequate amounts. Athletes should eat less fat so that less than 30% of their total energy needs are derived from fat. In general, dietary data on athletes revealed excessive fat intake (12).
Eating for, during and
after competition
Before and after intermittent,
high-intensity exercise, an athletes food intake should include easily
digested high-carbohydrate foods that are familiar and psychologically
satisfying.
The recommendations from
various studies for eating prior to any competition suggest that more than
200 g of carbohydrate from high-carbohydrate foods should be eaten 3-4
hours before competition/game to increase performance opportunities.
As the time approaches for competition/game, athletes may feel hungry and
should be able to consume food or drink containing carbohydrate (30-60
g) until 1 hour before competition. Athletes should be advised to
experiment with eating and drinking strategies on training days as opposed
to match/competition days so as to avoid any possible negative consequences
of pre-match ingestion.
Small carbohydrate feedings during endurance events of more than 1 hour may delay fatigue. Feedings should be at regular intervals to provide about 30-60 g carbohydrate every 60 minutes (13). Athletes should become comfortable with these feedings during their practice sessions. Athletes often find that consumption of carbohydrate-electrolyte containing sports beverage is better tolerated than solid foods during activity.
Carbohydrate consumption after exercise ensures repletion of muscle glycogen. Research shows that muscle will replete glycogen stores to a higher degree when up to 600 g of easily-digestible carbohydrate is consumed within the first two hours after exercise. The athlete should begin eating high-carbohydrate foods as soon as possible after physical exertion.
Fluid needs
The major causes of fatigue
during high-intensity, intermittent exercise are depletion of muscle glycogen
and/or dehydration. The consumption of a high-carbohydrate diet both
for training and for competition has already been referred to above.
With regard to fluid needs, athletes should be advised to drink water,
sports beverages or any other palatable fluids to meet personal hydration
needs and to avoid any level of dehydration that could impair physical
performance (9).
Sports nutritionist should encourage athletes to monitor their own individual fluid needs by weighing themselves prior to and after both training and competition. It is difficult and inappropriate to make specific recommendations due to the individual variability of sweat output during training or match-play or variability in temperatures. Obviously, warmer climates will promote a greater sweat output. Although general recommendation for fluid intake cannot be made, a very practical guideline for athletes is to drink fluids after exercise to regain any weight loss or until the urine is a very pale yellow in colour or clourless (14).
Vitamins and Minerals
Vitamins and minerals play
an important role in the metabolism of protein, carbohydrate, lipids and
muscle function. Although physical activity increases the need for
some vitamins and minerals, this increased requirement can typically be
met by consuming a balanced high-carbohydrate, moderate protein, low-fat
diet. Individuals at risk for low vitamin/mineral intake are those
who consume a low-calorie diet.
The common belief that if enough is good, more is better has probably been largely responsible for the continued use of massive doses of vitamins and minerals to improve athletic performance because of the belief that they have ergogenic properties. Although vitamin and mineral supplementation may improve the nutritional status of an athlete consuming marginal amounts of nutrients from food and may improve performance in those with deficiencies, there is no scientific evidence to support the general use of supplements to improve athletic performance (15-16).
Of the micronutrients, special attention to calcium and iron is necessary, especially for adolescence, and for all female athletes competing in events where body fat content is maintained at low levels. Amenorrhoeic women should be especially concerned over bone health and the need for an adequate dietary calcium intake.
Ergogenic aids
Compounds such as bee pollen,
caffeine, glycine, carnitine, lecithin and gelatin, are claimed, through
anecdotal evidence, to improve strength or endurance. Although popular
with some athletes because of this perceived ergogenic benefit, scientific
research has failed to substantiate the claims for these products.
However, because of the placebo effect, some athletes are convinced that
certain foods, dietary regimens or supplements improve performance.
These substances may provide certain psychological benefits rather than
proven physiological ones. However, when use of these substances
replaces a sound nutrition programme, health and performance may be compromised,
resulting in serious consequences.
References
![]()
|
|
THE
ROLE OF PHYSIOTHERAPY IN THE MANAGEMENT OF SPORTS INJURY
 |
Jane Susan Churme
Diploma in Physiotheraphy Physiotherapist Rehabilation Unit Hospital Universiti Sains Malaysia |
Introduction
In the past, management of sports injuries was taken lightly. With the change of time, the sports industry has grown and expanded so much so that our sports men and women has become an important commodity.
With this, the role of Physiotherapy in management of sports injuries has also gained importance. The role that a physiotherapist play is now not only a matter of application of certain modalities for specific symptoms but also entails a thorough examination, assessment, treatment planning and application as well as monitoring treatment effect together with modification of the treatment plan to suit the progression and condition of the athlete.
Principles of Management of Sports Injuries
The objectives are
Treatment Programme
RICE Regimen
This regimen is the most appropriate treatment of any soft tissue sports injury during the acute stage. Ice treatment should be continued up to 72 hours after injury.
The aim of RICE Regimen is to control swelling, reduce secondary damage as well as reduce pain and muscle spasm. This will aid in a more rapid recovery thus shortening the treatment period. RICE stand for:
R: Rest
the injured
part should be rested.
I: Ice
Application of ice pack/ice
cubes for 12 to 15 minutes.
Never apply
ice directly to skin.
Wrap the
injured area in a wet, conforming bandage or crepe, or cloth
(Dampness
assists cooling).
Place the
ice pack over the general area of the injury.
C: Compression
A heavy weight
crepe bandage is applied over the ice pack, beginning
distally extending upwards to the affected area.
Apply a heavy weight crepe bandage over the ice pack.
Check for continued circulation by briefly pinching them with finger
and thumb. The white colour should quickly return to normal.
Reapply the bandage reducing bandage tension if numbness or
bluish colour occurs at the extremities.
E: Elevation
The injured
part is elevated to above the heart level during ice application and rest.
Other treatment options
Following the acute phase (0-72 hours),
a physiotherapist has other treatment options to aid in recovery and rehabilitation
of the sports persons.
Electrotherapeutic Modalities (Pain Reduction)
1. Transcutaneous Electrical Nerve Stimulation
(TENS)
TENS is the application of low intensity,
pulsed, alternating or direct current, via surface skin electrodes and
is effective in reduction of pain of muscle sprains, ligamentous damage,
nerve root irritations and surgery.
TENS is effective for both acute and chronic
pain
2. Electro Acupuncture (EAP)
EAP is performed in conjunction with TENS
by applying an intense electrical stimulus to acupuncture points.
3. Interferential Therapy (IT)
It is based on the interference effect
when two medium frequency currents cross the patients tissue, resulting
in stimulation of motor and sensory nerves with much lower skin impedance.
It is used to reduce pain, stimulate deeply
placed muscles and assist in absorption of exudate, which reduce swelling.
4. Superficial Heat and Cold
Superficial topical heat applied via hot
baths, moist warm towels, water bottles, infrared lamps and hot packs is
useful in treatment of chronic pain and muscle spasm.
On the other hand, superficial topical
cold applied via ice bags, cold towels, ice massage and ice compresses
is selected for treatment of acute pain and swelling.
5. Deep Heat
a) Ultrasound
Ultrasound energy produces a number of
physiological effects, which makes it a useful agent for the management
of musculo-skeletal problems. These effects include
i. decrease in inflammation
ii. increase in extensibility of
connective tissue
iii.reduction of muscle spasm
b) Shortwave Diathermy (SWD)
When a suitable method of application
is chosen, SWD provides a deep form of heat. This enables a large body
part (back thigh) and deep areas (hip) to be treated more effectively.
These modalities assist in control of pain.
However, other treatment strategies are required to rectify the cause of
pain and dysfunction.
Prevention is Better than Cure!
Physical conditioning, maintainance of physical fitness and taping help in injury prevention. These can be archived through the following activities, where advise and guidance from a physiotherapist would be beneficial.
A) Streching or Flexibility Exercise
After a proper warm-up session prior to sport activities or competition, stretching or flexibility exercises should be performed to prepare the body for vigorous activity and reduce risk of injury.
AIM- To lengthen muscle and tendon tissue
- To increase range of motion at
a joint.
Effects
- Releases muscle tension
- Decreases risk of muscle tearing
- Improves muscle performance
- Increases mobility of a joint
Guidelines
- Warm-up first as this increases
stretchability.
- Do not bounce
Duration
- Maintain position for 15 seconds.
- Relax for 5 seconds and repeat
twice.
-Perform preparation for every training
and playing session.
- Perform also at the end of every
training and playing session to reduce muscle soreness and maintain maximum
length.
B) Muscle Strength, Endurance and Power.
Muscle strength and power stabilize and protect the joints. Strong and powerful muscles enhance the sport persons performance as well as help avoid risk situations.
When resistance is applied to a muscle as it contracts, the muscle will gradually become stronger over a period of time. As muscle strength increases, the cardiovascular response of the muscle improves so that muscular endurance and power also increases.
To increase strength of a muscle, the muscle contraction must be resisted so that increasing levels of tension will develop due to hypertrophy and recruitment of muscle fibres.
C) Taping for prevention and care of injuries
Rigid sports tape and clastic adhesive bandage contribute most to preventing injury when they are applied effectively.
Before taping remember:
i) Determine why
ii) Know the anatomy involved
iii) Decide how.
Some guidelines to remember when taping.
Place the joint to be supported in the
position that is best for protection and usage in play.
Start tape from a position and direction
that best allows it to follow the body contours, but can still go where
the specific job requires.
Commence all taping with anchor pieces,
which encircle above or below the joint to be supported.
Maintain moderate tape tension as it
is laid on to the skin.
Increase tension to any section of tape,
which acts to shorten the joints range of motion.
Avoid continuous taping use multiple
strips.
Overlap each piece by 1/2 to 3/3 over
the tape below.
Complete all taping procedures with
locking pieces (basically the same as anchors).
Practice makes perfect, so remember practice
is needed to gain skill in taping.
Conclusion
This brief article outlines the role that a physiotherapist has in sports injuries. At the present time not many of our sporting bodies have attending physiotherapist. In western countries, as their athletes are so highly regarded, the injuries are also taken very seriously and it is a must for them to undergo an extensive vigorous physiotherapy programme before they take a fitness test to allow them to continue with their sports activities.
Hopefully, this will also happen in Malaysia
so that our athletes will be more physically prepared.
![]()